Perioperative Risk, in Plain Sight
Patient safety is the first principle of anesthesia. Viali's new risk grade brings it to the surface of the daily workflow — and keeps it there, from pre-op through PACU.
TL;DR
Viali's Perioperative Risk Grade automatically synthesises risk data already in the chart and shows a single LOW/MEDIUM/HIGH chip — with the driving domain — on the patient card and across the whole perioperative chain. It is a summary, not a decision, and does not replace the anesthesia consultation.

Patient safety is the founding principle of anesthesiology. Every guideline — from the WHO Surgical Safety Checklist to the ASA and ESAIC pre-operative recommendations — converges on the same idea: anticipate risk before the patient enters the operating room, not after.
In practice, that anticipation is often diffuse. The information needed to grade a patient's perioperative risk — cardiac history, thromboembolic factors, pulmonary status, frailty, the planned procedure itself — is already in the chart, but it is spread across the intake questionnaire, the anesthesia assessment, the surgical plan, and the medication list. The clinician synthesises it on the fly, every time.
Viali's new Perioperative Risk Grade does that synthesis automatically, and surfaces it where the team already looks.
What it shows
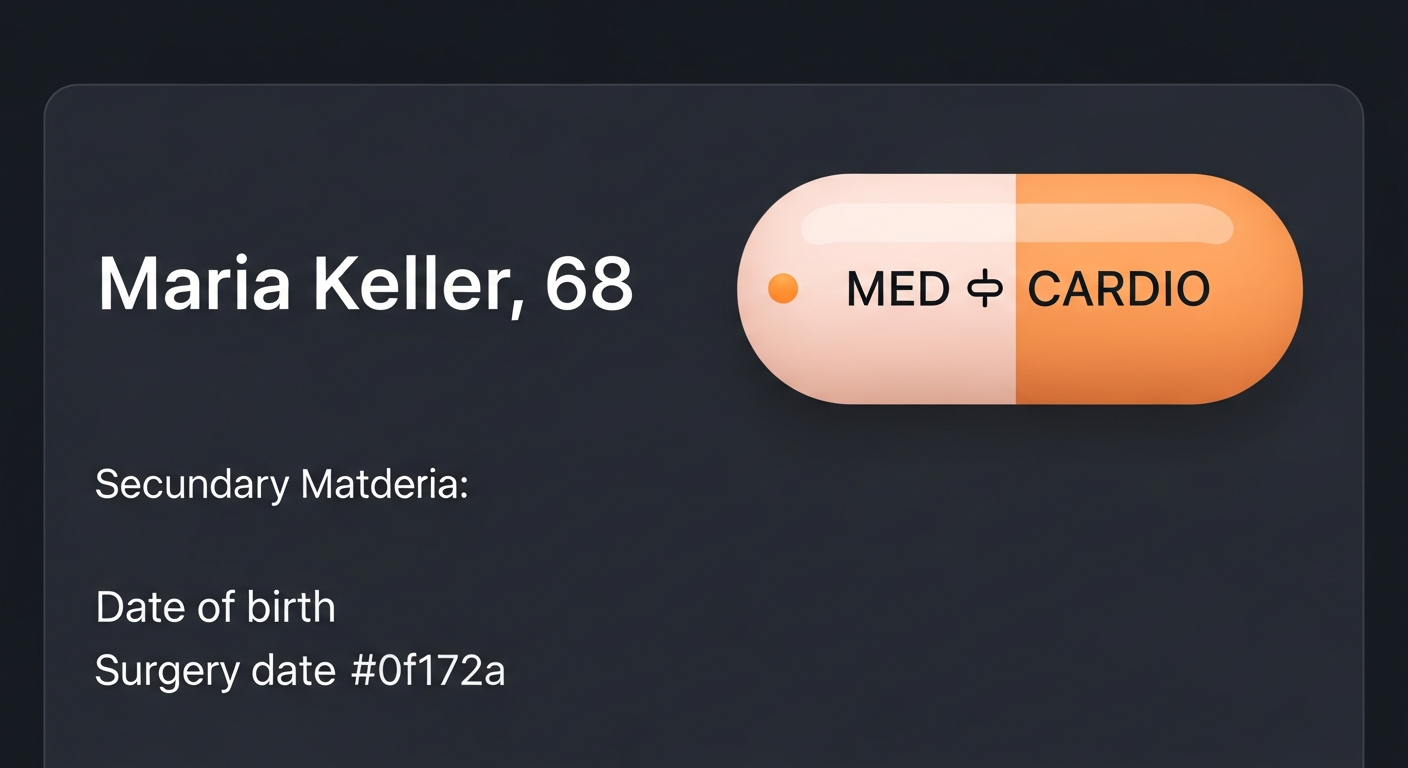
A single chip on the patient card classifies the case as LOW, MEDIUM, or HIGH risk, with the driving domain — cardiac, pulmonary, VTE, frailty, or surgical — named alongside the grade. The grade is computed from validated risk inputs already captured in Viali: comorbidity flags, age, surgery risk class, and anesthesia-specific findings.
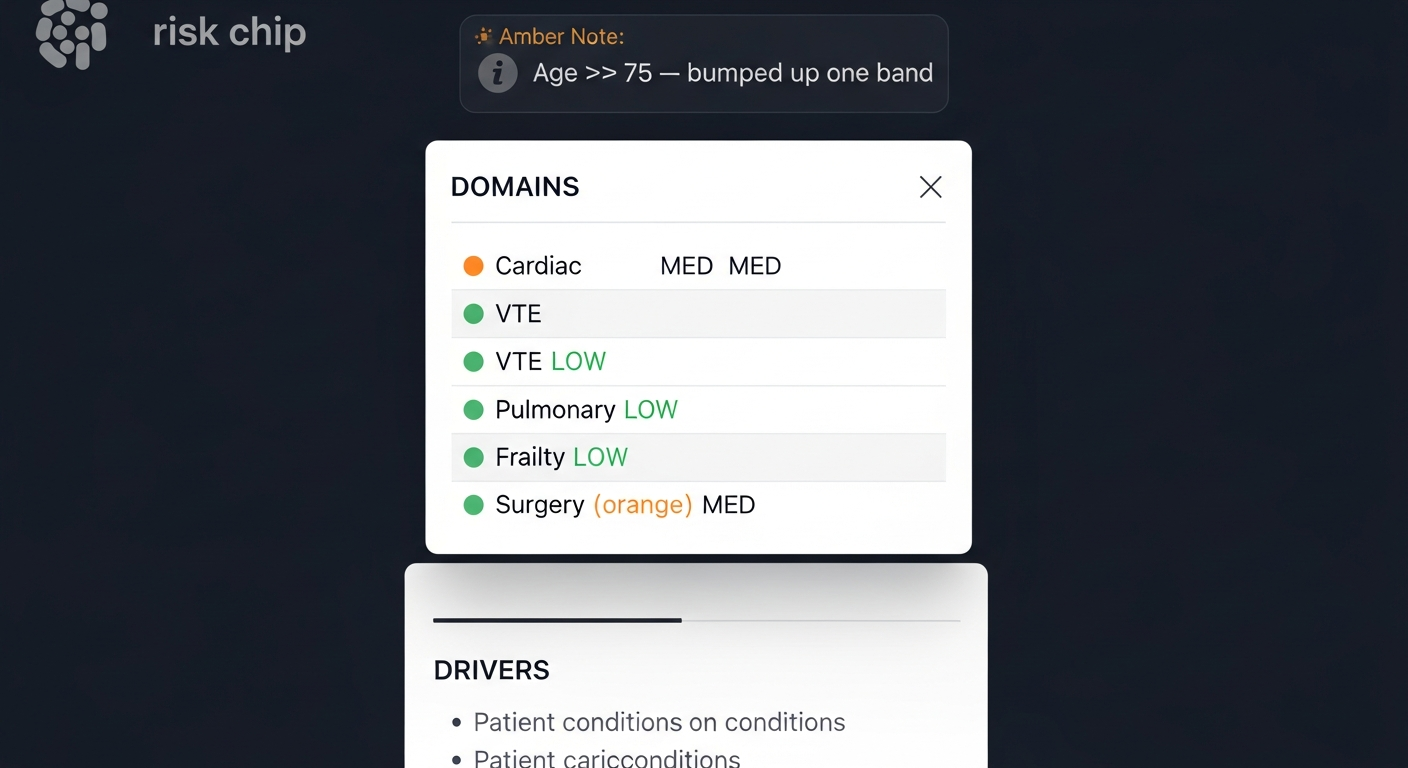
Clicking the chip opens a breakdown of the five risk domains, the specific drivers that contributed to the grade, and any modifiers — for example, the age-≥75 escalation that bumps the grade up one band for major procedures.
Why a "Preliminary" state matters
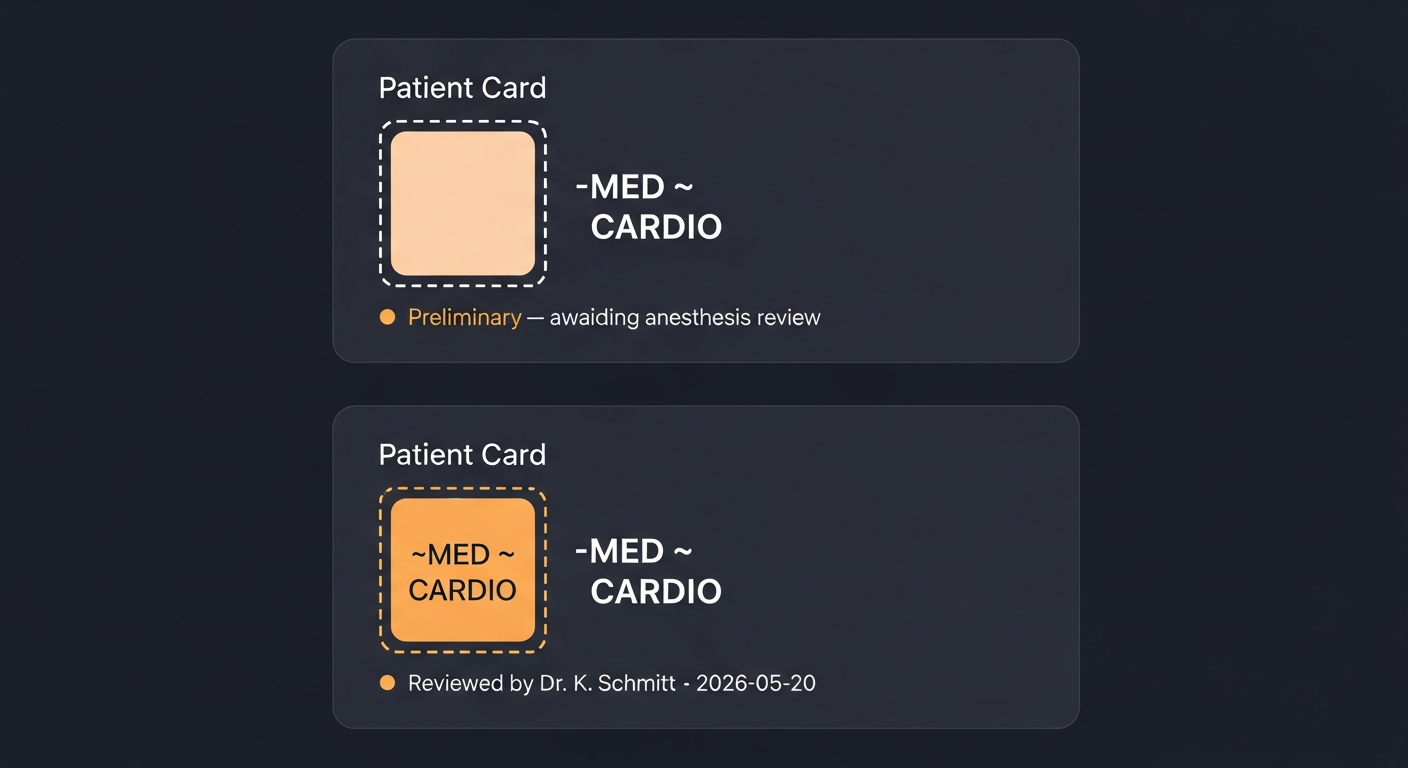
A risk grade computed from the patient questionnaire alone is not the same thing as a risk grade reviewed by an anesthesiologist. Viali makes that distinction explicit: when the grade is derived only from patient-supplied data, the chip is rendered with a dashed border and prefixed with a tilde (~MED).
The clinical meaning is unambiguous — this case still requires anesthesia review. Once the anesthesia pre-op assessment is filed, the chip transitions to a solid border, signalling that the grade now reflects clinician judgement.
Shared across the perioperative chain
A perioperative risk grade only delivers on its purpose if the entire team sees the same one — at every step of the patient's journey. Anesthesia is a relay: the pre-op anesthesiologist, the attending in theatre, the circulating nurse, and the PACU team each take custody of the same patient under different conditions. The cost of a risk factor lost between handovers is the same as the cost of one missed at intake.
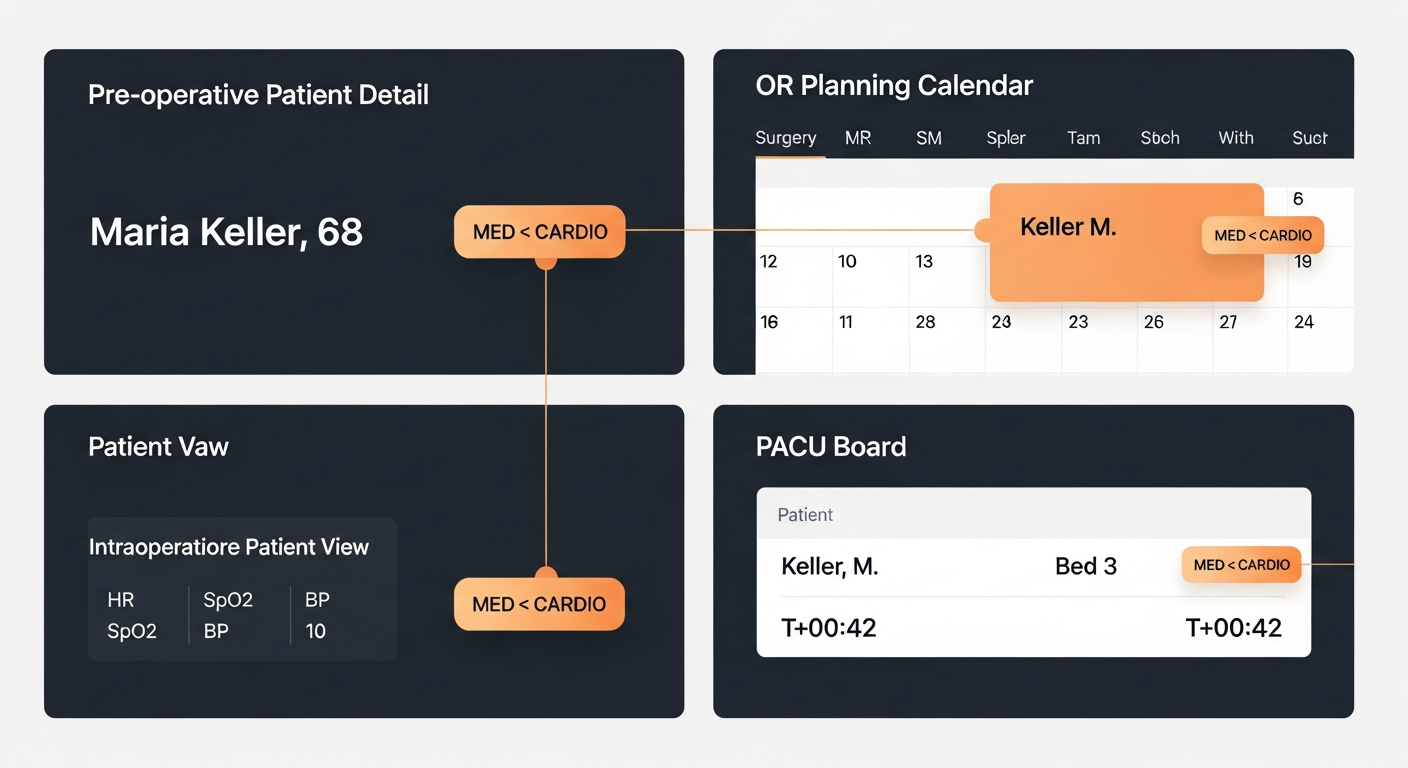
In Viali, the risk grade follows the patient through the full perioperative chain. The same chip — with the same grade, the same drivers, and the same modifiers — is visible in:
- the pre-operative patient record, during the anesthesia consultation;
- the OR planning calendar and surgery summary, on the day of operation;
- the intraoperative patient view, throughout the case;
- the PACU board, during recovery and until discharge.
There is no re-synthesis at every handover, no risk context lost between shifts, no quiet drift between what the pre-op anesthesiologist concluded and what the PACU nurse sees on her screen. The grade is computed once from the canonical chart data and shown everywhere — and any change to the underlying clinical record (a new diagnosis, an updated assessment) is reflected in the chip immediately, in every view.
What it does not do
The risk grade does not replace the anesthesiology consultation. It does not schedule, cancel, or alter clinical care. It is a *summary*, not a *decision*. Its purpose is to make the information already in the chart legible at the moment of triage — and continuously available through the perioperative chain — when each member of the anesthesia team is deciding how much attention this case needs *right now*.
In anesthesia, the cost of missing a risk factor is asymmetric. The cost of surfacing one redundantly is a glance. Viali's risk grade is built around that asymmetry.
Frequently asked questions
What does the perioperative risk grade show?
A single chip classifies the case as LOW, MEDIUM or HIGH risk, with the driving domain — cardiac, pulmonary, VTE, frailty or surgical — named alongside the grade.
How is the grade calculated?
It is computed from validated risk inputs already captured in Viali: comorbidity flags, age, surgery risk class and anesthesia-specific findings.
What does a preliminary (dashed) chip mean?
The grade was derived only from patient-supplied data and still requires anesthesia review. Once the pre-op assessment is filed, the chip switches to a solid border.
Where is the risk grade visible?
The same chip appears in the pre-operative record, the OR planning calendar and surgery summary, the intraoperative patient view, and the PACU board.
Does the risk grade replace the anesthesia consultation?
No. It is a summary, not a decision — it does not schedule, cancel or alter clinical care.
Does it need configuration?
No. The grade is computed automatically from existing patient and surgical data, in accordance with the hospital's regional clinical guidelines.
*Available now on all Viali deployments. No configuration required — the grade is computed automatically from existing patient and surgical data, in accordance with the hospital's regional clinical guidelines.*
Ready to experience this yourself?
Book a demo and see how Viali transforms your clinic operations.